


Improved
6141 HealthChanged
3797 LivesSaved
3584 Lives0 lives impacted in the last 24 hrs Learn More
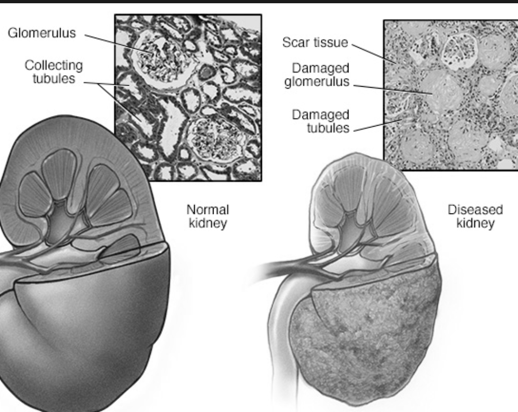
Women with kidney failure may not be getting enough dialysis treatment, according to several recent articles in the medical literature. With high efficiency membranes, dialysis can be accomplished with treatment three times per week, 2 to 4 hours per session. But is this enough?
Clearly, longer and more frequent dialysis sessions provide a better approximation to normal kidney function. But the patient's quality of life is adversely affected by spending too much time hooked to a machine. So from the beginning of the dialysis era, researchers have given considerable attention to finding the optimum treatment dosage.
The concentration of urea in the blood is the standard measure of dialysis results, not because it's the most important molecule to be filtered out, but because it's easy to measure and it diffuses quickly. Urea is distributed throughout the total volume of water in the body, to a reasonable approximation. A kinetic equation based on simplifying assumptions provides an index of dialysis effectiveness based on the efficiency of the dialysis membrane, the time of treatment, and the volume of water in the patient's body. This index is Kt/V, where:
K = rate constant for the dialysis machine,
t = time of treatment,
V = distribution volume for urea (volume of water in the patient's body)
As technology has advanced to make more efficient dialysis membranes, the time for dialysis treatment has decreased (higher K and lower t).
Body size is the standard parameter used to calculate dialysis dose for individual patients. The volume of water in the body can be calculated from weight, age, and gender. However, observational studies have shown that smaller patients have poor results relative to larger patients. Thus researchers have explored other parameters, and reported these results:
1. Calculations based on the mass of high metabolic rate organs would require a substantial increase in dialysis dose for both male and female patients with small body size.
2. Using liver size, predicted from liver-specific anthropometric equations, would require more dialysis for women of any body size.
3. Metabolic rate calculations give essentially the same results as body size calculations.
4. Calculations based on body surface area would require more dialysis for women of any body size, and for small patients of either gender. The theoretical basis for using body surface area is not well understood, but this parameter is easily calculated, and the results incorporate the benefits of considering both liver size and mass of high metabolic rate organs.
References:
Daugirdas JT et al, “Comparison of proposed alternative methods for rescaling dialysis dose: resting energy expenditure, high metabolic rate organ mass, liver size, and body surface area”, Semin Dial 2008 Sep-Oct;21(5):377-84.
Locatelli F et al, “Dialysis dose and frequency”, Nephrol Dial Transplant 2005;20:285-296.
Linda Fugate is a scientist and writer in Austin, Texas. She has a Ph.D. in Physics and an M.S. in Macromolecular Science and Engineering. Her background includes academic and industrial research in materials science. She currently writes song lyrics and health articles.
Add a CommentComments
There are no comments yet. Be the first one and get the conversation started!