


Improved
6141 HealthChanged
3797 LivesSaved
3584 Lives0 lives impacted in the last 24 hrs Learn More
My Austin phone book does not have a section for Nephrology under the Medical Specialty Guide heading, but we do have nephrologists here. Nephrologists specialize in diseases of the kidney, and overlap to some extent with their better known “cousins”, the urologists.
We all hear quite a bit about protecting our heart health, but not much about protecting kidney health. Two nephrologists would like to change that. They wrote a list of the top ten things they wish every primary care physician knew. Here is a summary of their paper in the Mayo Clinic Proceedings.
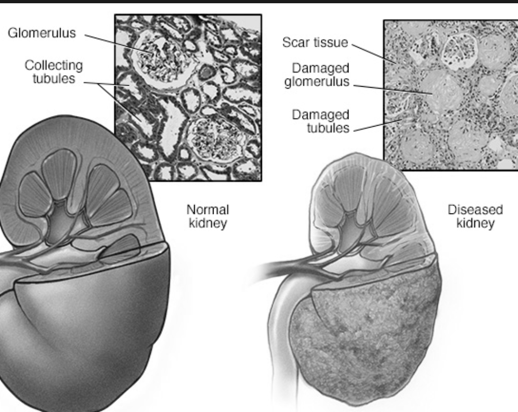
1. Normal creatinine levels in the blood do not guarantee healthy kidneys. This test is important in annual check-ups, but should be interpreted with caution.
2. Some medications spuriously elevate the creatinine level in the blood.
3. Patients with decreased glomerular filtration rate or protein in the urine should be evaluated to determine the cause. A positive urine dipstick test for protein should be followed up with a spot urine protein to urine creatinine ratio test.
4. In patients with early-stage chronic kidney disease, periodic evaluation and intervention are appropriate to slow the progression of the disease and avoid its complications. Drugs that cause kidney damage (such as NSAIDs, aminoglycoside antibiotics, and radiocontrast agents) should be avoided, and blood pressure should be controlled diligently.
5. Blood pressure medications (ACE inhibitors and angiotensin II receptor blockers) should not be automatically discontinued because of a small increase in the level of creatinine or potassium in the blood. Blood pressure, creatinine, and potassium are all important, and trade-offs have to be evaluated.
6. Anemia in patients with chronic kidney disease should be treated with erythrocyte-stimulating agents, but should not be overtreated.
7. Phosphate-containing bowel preparations (e.g. for colonoscopy) should be used with caution.
8. Patients with severe chronic kidney disease should avoid oral preparations containing magnesium or aluminum (e.g. Maalox and Mylanta).
9. Although most patients with high blood pressure should not be screened for secondary hypertension, certain clinical clues may suggest the presence of an underlying cause that may be treated to improve the patient's condition.
10. In patients with recurrent kidney stones, an in-depth metabolic evaluation is needed to identify and treat risk factors that can be modified.
Kidneys are just as vital as hearts. Let's take care of them!
Reference:
Paige NM et al, “The Top 10 Things Nephrologists Wish Every Primary Care Physician Knew”, Mayo Clin Proc 2009 Feb; 84(2): 180-186.
Linda Fugate is a scientist and writer in Austin, Texas. She has a Ph.D. in Physics and an M.S. in Macromolecular Science and Engineering. Her background includes academic and industrial research in materials science. She currently writes song lyrics and health articles.
Add a Comment1 Comments
Hi Linda - What a great idea! If every specialist group developed a "Top 10" list for internists, family practitioners, nurse practitioners and others who are usually the first healthcare provider a patient sees, it would benefit everyone and speed up the diagnosis, treatment and recovery processes. The data could be kept on a website, managed by a peer reviewed committee and regularly updated. I love this idea, and hope the Austin nephrologists will take the concept further. Thanks for sharing. Pat
December 5, 2009 - 12:47pmThis Comment